We had lecture all morning and covered:
- Scene size up and patient assesment
- Wound management
- Cold injuries
- Heat injuries
- Lighting
- Water purification
- High velocity injuries
- Water disinfection
We went outside for the afternoon and practiced some patient scenarios (which are always total bull shit, but I guess they serve a purpose). This, I might add is where the EMTs and Paramedics shined. The MDs were a little out of their element. Scene size up what!? Obviously, to graduate from medical school and complete a residency you have to have an incredible depth of knowledge. However, when it came to extricating 'patients', carrying, or log rolling things didn't go do well. I learned from them, they learned from me, we're all friends!
As I sign off, I'd like to leave you with some interesting lightning facts (THE most interesting lecture of the day):
- The most likely time for a severe lighting strike is before the storm appears and after the storm has passed
- Rubber boots, rubber tires... they don't mean shit when faced with a unidirectional massive current impulse of 30 million volts. If it traveled 10 miles through the air it'll blow through rubber like nothing
- For those of us in EMS...A mass casualty incident (MCI) involving a lighting strike should be reverse triaged. Patients may appear dead because the heart initially becomes asystolic after the strike. It will, however begin beating again. There will often be a concomitant respiratory arrest that occurs and the heart may deteriorate back into asystole secondary to the respiratory arrest. This respiratory arrest may last 5-8min (during with the patients is asystolic and apnetic) because of a temporary paralysis of the medullary center. -Long story short, keep them alive and they'll be fine (even if they look dead). If the patient looks ok and is at least semi alert and oriented they'll be fine- take care of the serious patients first.
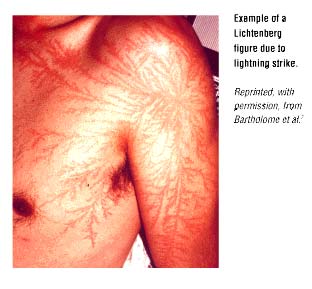 I would totally get one as a tatoo if I ever got hit (as opposed to that OTHER tatoo I was thinking of getting, more of that later).
I would totally get one as a tatoo if I ever got hit (as opposed to that OTHER tatoo I was thinking of getting, more of that later).Cheers!

4 comments:
Who says trauma can't be beautiful?
Cool! i had a question about the lightening strike on a pratice test and found it really amazing...you should get that tatoo anyway...thanks for sharing you advertures with us.
So, c'mon, you know you want to tell...what is the "other tatoo"...??
Lucid: When it goes smoothly it can be ;). Things went much better today during our practicals (mainly because I had a great team: crusty ER doc, rural PA/EMT, Inernist, OB/GYN, and myself.
Tracy: Time will tell... time will tell =P
Lightening strikes...another reason to never wear an underwire bra ;)
At a wilderness med conference a couple of years ago I saw an RN present on her job--which is to travel around the US and manage the lightening strike cases in hospital and gather data on the actual events. It was one of the most fascinating presentations I've ever seen. Yet another job they never tell you about when you want to drop out of high school!
Post a Comment